
working to improve care for people living with:
By now you probably know that very few doctors in Ontario have experience diagnosing or treating ME/CFS. Many may not even accept that it is a real medical condition. This is where the (Canadian) Centre for Effective Practice or CEP comes in. It has created a tool to help family physicians recognize, assess, diagnose and treat ME/CFS. To access the tool click on the blue button: CEP Tools for ME/CFS.
The CEP is a Canadian group focused on helping Canadian primary care clinicians (like your family doctor) “navigate the increasingly complex clinical environment”. In other words they offer Canadian doctors guides to cope with the ever-changing world of medical practice. A great example of this is the aforementioned “tool” designed to help your doctor diagnose and treat ME/CFS -a condition that most doctors don’t know much about.
The CEP has also prepared a list of resources for both patients and clinicians. Click on the respective blue buttons for copies of these resources.
Myalgic encephalomyelitis (ME) is a chronic, complex multi-system disease. It is also known as ME/CFS and still commonly, as chronic fatigue syndrome. ME is what CareNow Ontario will use unless we are quoting from a source using a different terminology. ME has diverse symptoms and impairments, across many body systems, including neurological, immunological, autonomic and energy metabolism. The hallmark symptom is post-exertional malaise (PEM), a delayed (hours or days) exacerbation of symptoms following even minimal effort or activity of any kind.
Other typical symptoms include loss of stamina, debilitating fatigue, cognitive impairment (difficulty thinking or concentrating, ‘brain fog’), unrefreshing sleep, and autonomic manifestations such as orthostatic intolerance. Also common are musculoskeletal and joint pains, headaches and sound, light and chemical sensitivity. Fatigue is only one amongst a wide variety of symptoms.
ME affects many people of all ages, in Canada and worldwide. In Ontario, the number affected in 2016 (the last year for which we have Ontario-specific numbers) was 250,000 or just over 2% of the population (12 and over) with the majority (approximately 65%) of those being women. While these statistics do not include children, there is evidence that ME affects children.
Onset can be sudden, following a viral or other infection but it can also occur more gradually, as well as after other events, such as environmental exposures. ME occurs with a wide range of severity, with some people being ‘relatively’ mildly impacted but still with serious consequences for their quality of life and economic security, unable to undertake daily activities in a consistent manner or to work; while others, estimated to be 25% are severely or very severely affected, often housebound or bedbound.
Researchers are actively working to unravel the causes of ME and to develop effective treatments. Medical schools have not yet incorporated ME into their curriculum, so very few providers have trained to recognize/diagnose or to treat ME; this despite there being accepted diagnostic criteria that are widely available and, even without all the answers, some treatments that can be provided on a symptomatic basis.
There is a significant subset of people with long COVID who share many symptoms of ME, including post-exertional malaise, and are meeting ME case definitions. This is of great significance for both people with long COVID and those with ME. On the long COVID side, many of the treatments that have been offered to provide symptomatic relief for ME may help long COVID. Additionally, armed with knowledge gained from the ME experience, greater caution may be used in applying treatments, such as graded exercise therapy, that have not helped, and in fact have harmed people with ME. And from the ME side, the significant amount of research now ongoing into long COVID may be helpful for ME (and for other conditions such as FM and ES-MCS), should the underlying mechanisms be found to have a common basis.
The need is great, that’s why CareNow Ontario is working to bring care and education into being.

Myalgic encephalomyelitis is an acquired neurological disease with complex global dysfunctions. Pathological dysregulation of the nervous, immune and endocrine systems, with impaired cellular energy metabolism and ion transport are prominent features.
Myalgic Encephalomyelitis involves dysfunction across at least thirteen major biological systems with substantial mechanistic interdependence. Mitochondrial energy deficit drives neuroinflammation and oxidative stress while impairing immune cell function. Chronic immune activation and altered cytokine production perpetuate neuroinflammation despite simultaneous immune exhaustion. Dysregulation of the HPA axis and autonomic nervous system, driven by activated immune-inflammatory pathways, causes cardiovascular and metabolic dysfunction. Vascular and endothelial abnormalities reduce tissue oxygenation, compounding mitochondrial dysfunction and perpetuating the bioenergetic crisis. Gut dysbiosis permits microbial translocation triggering sustained immune activation. Persistent or reactivated viral infections establish latency-based immune evasion mechanisms. These systems interact through feedback loops—cellular energy deficit amplifies inflammation, inflammation exacerbates oxidative stress, oxidative stress damages mitochondria—creating self-sustaining pathophysiological cycles that characterize ME/CFS’s chronic, relapsing-remitting course.
CareNow Ontario will use the term Myalgic Encephalomyelitis (ME) on this website and in associated documents, unless specifically referencing a document that uses a different term. Over the years other terminology has been used (e.g., ME/CFS, chronic fatigue syndrome). The use of ME is in keeping with patient preference and the terminology that has been adopted by the ICanCME Research Network.
Myalgic encephalomyelitis (ME) stands for “muscle pain” and “inflammation of the brain and spinal cord.” ME is a serious, complex and debilitating condition causing a wide range of symptoms. It affects many people in Ontario and worldwide. In spite of recent research clearly demonstrating many biological abnormalities across many body systems, people living with ME face lingering stigma, in part because the underlying mechanisms of the disease are not known and a lack of funding for research has perpetuated this lack of knowledge. The name by which it has long been known, ‘chronic fatigue syndrome’ is another major reason for stigma.
Chronic fatigue syndrome was the name given to the illness in 1988 by a group convened by the Centers for Disease Control and Protection (CDC) to come up with a research definition for the bewildering ‘new’ illness that had resulted in outbreaks in Lake Tahoe, Nevada and in New York State. This became known as the Holmes criteria, or as the CDC 1988 criteria, for chronic fatigue syndrome. The chronic fatigue syndrome name was chosen as it was felt that ‘chronic fatigue’ amongst all the other symptoms present best defined the illness. This name was retained when the criteria were revised in 1994, also by a large working group convened by the CDC in what became known as the Fukuda criteria for chronic fatigue syndrome. Neither the Holmes nor the Fukuda definitions were intended for clinical purposes.
Myalgic encephalomyelitis (at that time being called benign myalgic encephalomyelitis) first appeared in the medical literature in the mid 1950s. The disease described a complex illness with a variety of symptoms including tender lymph nodes, malaise, sore throat, muscle pain and signs of encephalomyelitis. In 1969, benign myalgic encephalomyelitis was added to the International Classification of Diseases (ICD) in the neurological category (diseases of the nervous system) as an included term to post-viral fatigue syndrome and there it remains, although the benign has been dropped. In 1970 an influential paper out of the UK suggested that this condition (at least that experienced in the outbreak at the Royal Free hospital in 1955) was epidemic hysteria. This paper continued to influence thinking about the illness as being psychogenic in origin for many years, even though the hysteria hypothesis was discredited as more and more biological abnormalities were found.
Although this is skipping ahead in the timeline, in 2011 a group of international experts created a consensus case criteria for myalgic encephalomyelitis (ME), using the Canadian Consensus Criteria for ME/CFS as the starting point but breaking with the use of ‘chronic fatigue’ in the name of the disease, citing reasons we’ll get back to later.
When the IOM/NAM wrote their report (2015) they proposed a new name for the disease — Systemic Exertion Intolerance Disease (SEID). They picked this name for several reasons:
The Institute of Medicine (IOM) (now the Academy of Medicine) in their 2015 ground-breaking report “Myalgic encephalomyelitis /Chronic fatigue syndrome: redefining an illness” noted that using the name chronic fatigue syndrome for the illness resulted in “trivialization and stigmatization for patients afflicted with this illness” and should not be used.
In ME/CFS the fatigue is different. “It’s not the fatigue that someone who is completely healthy might feel if they were just tired. It’s a very different, complex, and much more severe picture in ME/CFS.” Beth Pollack, Research scientist at MIT specializing in chronic diseases.
No other fatiguing disease has ‘chronic fatigue’ attached to its name – e.g. cancer/chronic fatigue, multiple sclerosis/chronic fatigue – except ME/CFS. Fatigue in other conditions is usually proportional to effort or duration with a quick recovery and will recur to the same extent with the same effort or duration that same or next day.
In ME/CFS fatigue does not manifest in way it does in other fatigueing diseases. In many cases the fatigue experienced is not proportional to effort, the recovery is not quick and there is a “reduced ability to undertake the same activity within the same or several days.
ME is the term the Canadian Institutes of Health Research-funded Canadian research network ICanCME uses. Just as ME/CFS supplanted ‘chronic fatigue syndrome’ in US government institutions and may be poised to do the same in the UK, many patients along with a number of researchers and clinicians are working toward ME being broadly accepted.
There are some who would like to see a name chosen that focuses more on the post-viral or multi-systemic nature of ME/CFS. A very significant proportion of those with “Long Covid” meet the diagnostic criteria for ME/CFS. Long Covid is recognized as being a complex multi-system disorder. There is a growing recognition within the scientific community that ME/CFS is also a complex disorder that may involve multiple systems as well.
However, Chronic Fatigue Syndrome (CFS) is still very much in use, so just because we use ME doesn’t mean everyone does.
Chronic fatigue syndrome is the term used by the pertinent service and diagnostic codes within the OHIP billing system (how doctors get paid), so it is very possible that if you get a diagnosis in Ontario your doctor, unless they have had specialized training, will use the term ‘chronic fatigue syndrome.’
CFS is what the doctors know and this is what the diagnosis and billing code system says should be used.
ME/CFS is also a term that is used by some, including those in advanced practice: it bridges between the term in the billing system and ME. The Task Force on Environmental Health made a recommendation that the billing and diagnostic codes be updated to include myalgic encephalomyelitis/chronic fatigue syndrome but this has not yet been acted upon.
The cause or causes of ME are still unknown. However, ME is increasingly viewed as an infection-associated chronic illness. This is because of the frequency of its association with infection -most people end up with ME after an infection- and the symptom overlap with illnesses following known infections like “Long Covid”. Perhaps half of those with “Long Covid” now meet the diagnostic criteria for ME.
However; other factors may also contribute to development of ME.
Some patients report experiencing an accident, trauma, immobilization, surgery, vaccination, or significant physical or emotional stress prior to onset of ME symptoms.
ME/CFS onset can be acute or gradual. Gradual onset can occur over months or years.
Acute onset may follow:
It should be noted that the re-emergence of an EBV infection may be a consequence of the illness and not the cause.
The percentage of ME/CFS patients who recover is not well-studied. However, there is evidence and experience that early diagnosis and timely and appropriate management may play a role.
Some patients return to full function. Many who improve continue to have symptoms but do not achieve pre-illness levels of function. Others who improve continue to modify their activities to remain improved or free of symptoms. Remissions occur but can be followed by relapses. Some symptoms do not improve or, in fact, worsen over time.
More studies are needed. However, most experts agree that children and teenagers have a better chance of full or partial recovery from ME/CFS than adults.
The severity and frequency of symptoms varies among patients and by individual patient. Symptoms can fluctuate during the day, from day to day, and throughout the illness.
ME ranges from mild to severe. Some patients may not appear obviously ill during clinical evaluations. Others with severe ME or exacerbated symptoms may not be able to visit the clinic. Healthcare providers may not see patients when their symptoms are at worst. Levels of illness severity are based on the patient’s degree of impairment:
Patients may be able with careful planning and activity management to keep a job or continue education. Patients may be able to participate in social and family activities and attend to daily life.
Patients might have trouble maintaining a regular work schedule. They may have difficulty standing and sitting for prolonged periods. Patients have limited ability to participate in social and family activities.
Patients may be wheelchair-dependent, house- or bed-bound for months or even years. Symptoms may increase after daily tasks or trips to healthcare providers. For example, bathing and cooking meals may require significant assistance. They may also need to adjust or interrupt their employment or education.

People who are severely affected are too sick to show up at doctors’ offices and have largely been invisible to the health system. And yet their numbers are estimated to be 25% of the ME population. Their needs are immense. They are housebound or bed bound. The most severely affected of those are:
They often need help with basic activities like eating, toileting, moving about (if they can even do that).
It is only relatively recently that more attention has been placed on what their needs are and how to provide medical and social care.
Very severely affected ME/CFS patients experience profound weakness, almost constant pain and severe limitations to physical and mental activity. They may also have hypersensitivity to light, touch, sound, smell, medications and certain foods.
These patients often cannot make office visits due to the severity of their symptoms. They require in-home assistance and management plans specifically adjusted to their needs by a coordinated care team of providers.
Caregivers, who provide management and the majority of care for patients, often have substantial stress and may need additional support.
The subset of severely ill ME/CFS patients who are completely bedbound requires special attention. They need in-home visits and phone/online check-ups, and a modified approach to activity management.
Some accommodations for those severely ill from ME/CFS include recumbent wheelchairs, portable cook surfaces, shower chairs and bedpans. These tools allow them to consider sitting when cooking or showering. They can use a bed-side commode instead of walking to the restroom. And they can take frequent breaks during activity to save their energy.
A realistic goal with severely ill patients is focusing on reducing stiffness and maintaining joint range of motion. This can be accomplished by passive range-of-motion exercises and gentle stretching (if touch can be tolerated). Hand stretches and picking up and grasping small objects may be all that can be managed by some patients.
These patients often cannot make office visits due to the severity of their symptoms. They require in-home assistance and management plans specifically adjusted to their needs by a coordinated care team of providers.
Sources
Montoya JG, Dowell TG, Mooney AE, Dimmock ME, & Chu L. went a step further writing this letter:
Letter to Healthcare Professional: “Caring for People with Severe ME/CFS” 6 October 2021
There are many conditions that are co-morbid (can co-exist) with ME and, where present, usually mean an increased symptom burden. It is important to recognize these co-morbid conditions.
Fibromyalgia, a common co-morbid diagnosis is an example as it can increase the muscle pain experienced. Identifying and appropriately treating co-morbidities can improve quality of life.
Just to give a small sample of conditions co-morbid with ME:
From the US ME/CFS Clinician Coalition: “Diagnosing and Treating Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)” (page four) “Identifying Commonly Comorbid Conditions”.
“In the past, a diagnosis of ME/CFS was made by first excluding all other possible conditions. However, the 2015 National Academy of Medicine report established ME/CFS as a positive diagnosis that can coexist with other conditions, including those in the differential diagnosis.
Recognizing co-morbid conditions early and treating them appropriately may improve the patient’s health, function, and quality of life.”
Postural Orthostatic Tachycardia Syndrome (POTS),
Neurally Mediated Hypotension (NMH),
Orthostatic Hypotension
Fibromyalgia,
Ehlers-Danlos Syndrome,
Tempomandibular Joint Dysfunction,
Sicca Syndrome (dry eyes/mouth)
Sensory Hypersensitivities (light, sound, touch, odors or chemicals),
Poor Balance,
Migraine Headaches,
Peripheral Neuropathy,
Small Fiber Neuropathy
New or worsened allergies,
Mast Cell Activation Syndrome,
Multiple Chemical Sensitivities,
Chronic infections,
Immunodeficiencies
Food Allergy and Intolerances, including to milk protein,
Gut motility issues,
Celiac Disease,
Irritable Bowel Syndrome,
Small Intestinal Bacterial Overgrowth
Hypothyroidism,
Hypothalamus-Pituitary- Adrenal Axis dysregulation (low normal or flattened cortisol curve),
Metabolic Syndrome
Sleep Apnea,
Restless Leg Syndrome,
Periodic Limb Movement Disorder
Secondary Anxiety,
Secondary Depression
Endometriosis,
Premenstrual Syndrome,
Vulvodynia
Interstitial Cystitis,
Overactive Bladder,
Nutritional deficiencies,
Vitamin B12 and D deficiencies,
Obesity
Click on the download button for a printable list of these conditions.
The same list was published in a supplemental table along with the following article:
Bateman L, Bested AC, Bonilla HF, Chheda BV, Chu L, Curtin JM, Dempsey TT, Dimmock ME, Dowell TG, Felsenstein D, Kaufman DL, Klimas NG, Komaroff AL, Lapp CW, Levine SM, Montoya JG, Natelson BH, Peterson DL, Podell RN, Rey IR, Ruhoy IS, Vera-Nunez MA, Yellman BP. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Essentials of Diagnosis and Management. Mayo Clin Proc. 2021 Nov;96(11):2861-2878. doi: 10.1016/j.mayocp.2021.07.004 Epub 2021 Aug 25. PMID: 34454716. supplemental table 1 scroll down until you reach Supplemental table 3 entitled: Conditions Which Commonly Co-exist with ME/CFS.
ME does occur in young children but is more common in adolescents. Because there has been very little research specific to children, we know less about it in that population than in the adult population. Less doesn’t mean we know nothing though and there was a specific chapter of Pediatric research in the 2015 US Institute of Medicine (now National Academy of Medicine)’s major report, Beyond ME/CFS: Redefining an Illness which is cited below:
Committee on the Diagnostic Criteria for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome; Board on the Health of Select Populations; Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. Washington (DC): National Academies Press (US); 2015 Feb 10. PMID: 25695122.
We also have a sense of the prevalence in children from a 2020 community-based study out of the US. It found the prevalence was .75% (or 75 out of 10,000). This may not seem like a lot but in every 200 children it means it is likely more than one of them will have ME.
As with adults, ME can occur gradually or acutely (following infectious mononucleosis is a classic example in adolescents). Similar to adults there is a wide range of severity. An excellent primer on Diagnosis and Management in young people was prepared by experienced ME clinicians in 2017. See the citation with a link below:
Rowe PC, Underhill RA, Friedman KJ, Gurwitt A, Medow MS, Schwartz MS, Speight N, Stewart JM, Vallings R, Rowe KS. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Diagnosis and Management in Young People: A Primer. Front Pediatr. 2017 Jun 19;5:121. doi: 10.3389/fped.2017.00121.
The range of symptoms in children is similar to adults and diagnosis can be made using the same criteria. Although this is the case some symptoms seem to be more common in children than in the adult population, such as orthostatic intolerance.
In children there are the additional complications of educational and social development issues. Educational accommodation is often required. It is important that teachers and administrators understand that ME is a medical disease that can result in difficulties with school attendance or an inability to participate in physical activities due to exertion intolerance – it not the result of an unwillingness to participate.
Fortunately, in addition to the 2017 Primer on Diagnosis and Management, [link again if you think it is needed] there are helpful resources available through a number of places. We’ve linked to some of these below.le
More websites devoted to children with ME/CFS.
Centers for Disease Control and Prevention (CDC):
American Myalgic Encephalomyelitis and Chronic Fatigue Syndrome Society:
The Solve ME/CFS Initiative:
The Teach-ME sourcebook from the National ME/FM Action Network is a valuable resource for parents and teachers.
The diagnostic criteria described below all try to define what is meant by the fatigue experienced by people with ME/CFS. Imagine that -all of a sudden- one has the energy level one associates with having the ‘flu or a bad cold or even pneumonia. Indeed ME/CFS often follows a conventional illness like a viral infection that leaves one feeling exhausted. However, after the infection has been cleared up one’s energy does not come back. You are as tired as you were when you were “sick” even though the sickness has passed. There are many variations on this theme. Onset might be slower and not follow an infection. One might recover some of the “pre-sickness” level of energy but not all of it. This new level of fatigue is not alleviated by sleep. The upshot is that you simply cannot do the things you used to be able to do. This unusual level of fatigue must continue for at least six months to meet the diagnostic critereia for ME.

PEM is a hallmark of ME/CFS. It involves fatigue and other symptoms that are disproportionate to the level of exertion of the activity that preceeded it. Since fatigue is already a symptom of ME/CFS PEM can be described as a significant worsening of symptoms following a level of exertion that the patient might might well believe was safe for them to engage in.
The “malaise” may set in almost immediately but is more commonly experienced a day or two after the exertion. It can last for hours, days, weeks, or months and is often described as a crash. People with ME/CFS need to know what level of exertion they can engage in such that it does not cause a bout of PEM. It is common for people with ME/CFS to use the term “energy budget” to describe what they are capable of. This budget is determined by how much exertion the person can engage in without triggering a “crash” or “PEM”.
PEM can also include worsening of the other common symptoms associated with ME/CFS.
The “gold standard” test for PEM is a two-day CPET (cardiovascular exercise test). The first test (day 1) establishes a patient’s baseline functional capacity while also serving as a stressor that leads to PEM. The test on day 2 measures how severe the induced post-exertional symptom flare is. If you have ME chances are that on day 2 you will be exhausted beyond what one should expect from the exertion on day 1. The downside of this diagnostic tool is that patients may not recover for days, weeks, or months.
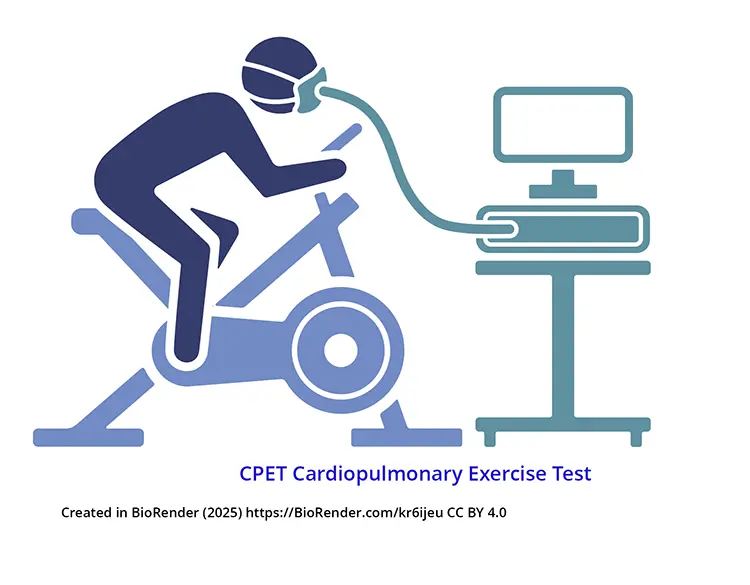
In the US a full 2 day CPET test must be carried out in order to earn a diagnosis of ME/CFS for the purposes of being granted a disability pension.
This is sometimes referred to as Sleep Dysfunction. Sleep no longer leaves one feeling refreshed or no longer alleviates fatigue. Sleep patterns may change.
This includes difficulties associated with thinking. Thinking becomes more difficult. Attention wanders. It is harder to process new information than it used to be -learning becomes more difficult.
Some describe experiencing “brain fog”.
Perhaps a good way to describe it is how hard it is to think (about just about anything) when experiencing extreme sleep deprivation without actually being sleep deprived. Think of it as brain fatigue.

This is how the CDC describes it.
Symptoms related to orthostatic intolerance, such as dizziness, fainting, heightened fatigue, cognitive difficulties, headaches, or nausea, are aggravated when maintaining an upright posture (either standing or sitting) in daily activities, and improve (though not always completely) when lying down.
Since there are no biomarkers that can be used in clinical practice diagnostic criteria have been arrived at by the consensus of experts. Clinicians will assess your symptoms against a case definition — a set of criteria specific to the disease, to see if you fulfill the requirements for a diagnosis. There are a number of case definitions that have been used over the years to diagnose ME.
The 2015 Institute of Medicine (IOM) Diagnostic Criteria for ME/CFS is used by the CEP and the CDC so if you live in Ontario these are the criteria that will apply to you. The other most commonly used set of criteria are the “CCC” (2003 Canadian Consensus Clinical Case Definition of ME/CFS). The obvious advantage of the 2015 IOM criteria is that it is simpler making it easier for doctors to make a diagnosis. The CCC is more often used when identifying ME/CFS patients for research purposes.
Plus at least one of the two following manifestations:
Frequency and severity of symptoms should be assessed. The diagnosis of ME/CFS should be questioned if patients do not have these symptoms at least half of the time with moderate, substantial or severe intensity. Source: Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness 2015 US Institute
Patient must have a marked degree of new onset, unexplained, persistent or recurrent physical and mental fatigue that substantially reduces activity level
There is a loss of physical and mental stamina, rapid muscular and cognitive fatigability, post-exertional fatigue, malaise and/or pain, and a tendency for other symptoms to worsen. There is a pathologically slow recovery period (i.e., it takes more than 24 hours). Symptoms are usually exacerbated by stress of any kind.
There is unrefreshed sleep or sleep quality and rhythm disturbance.
There is a significant degree of myalgia. The pain can be experienced in the muscles, joints, or neck and is often migratory in nature. Often, there are significant headaches of new type, pattern, or severity.
Two or more of the following difficulties should be present:
1 confusion, impairment of concentration and short-term memory consolidation,
2 disorientation, difficulty with information processing, categorizing and word retrieval, intermittent dyslexia, perceptual and sensory disturbances, and ataxia.
3 There may be “overload phenomena”: informational, cognitive and sensory, and/or emotional overload, which may lead to “crash” periods and/or anxiety. [Crash refers to a temporary period of immobilizing physical and/or cognitive fatigue.]
Orthostatic intolerance such as neurally mediated hypotension (NMH),
Postural orthostatic tachycardia syndrome (POTS),
Delayed postural hypotension,
Vertigo,
Lightheadedness,
Extreme pallor,
Intestinal or bladder disturbances with or without irritable bowel syndrome (IBS) or bladder dysfunction,
Cardiac arrhythmia,
Vasomotor instability, and
Respiratory irregularities.
Loss of thermostatic stability,
Heat/cold intolerance,
Anorexia or abnormal appetite,
Marked weight change,
Hypoglycemia,
Loss of adaptability and tolerance for stress,
Worsening of symptoms with stress and slow recovery and emotional lability.
Tender lymph nodes,
Recurrent sore throat,
‘Flu-like symptoms,
General malaise,
New sensitivities to food, medications and/or chemicals.
The illness persists for at least six (6) months. It usually has a distinct onset, although it may be gradual. Preliminary diagnosis may be possible earlier. Three months is appropriate for children. To be included, the symptoms must have begun or have been significantly altered after the onset of the illness. It is unlikely that a patient will suffer from all symptoms in Criteria 4 and 5.
The manifestations fluctuate and may change over time. Symptoms can exacerbate with stress, resulting in a slow rate of recovery. Children may experience numerous symptoms of similar severity, but their hierarchy of symptom severity tends to vary from day to day.
Source: Carruthers BM, Jain AK, De Meirleir KL, Peterson DL, Klimas NG, Lerner AM, Bested AC, Flor-Henry P, Joshi P, Powles ACP, Sherkey JA, van de Sande MI. Myalgic Encephalomyelitis/chronic fatigue syndrome: Clinical working case definition, diagnostic and treatments protocols. J Chronic Fatigue Syndr. 2003;11:7–115
There are a number of case definitions that have been used over the years. Five of these case definitions are discussed below.
The Centers for Disease Control and Prevention coordinated the development of a case definition for what was being termed ‘chronic Epstein-Barr virus syndrome’ in 1988 and its update in 1994. The 1988 definition by Holmes and colleagues was the first use of the name ‘chronic fatigue syndrome,’ chosen because “chronic or recurrent debilitating fatigue” was what primarily characterized the symptom complex. This terminology was retained in the update.
The 1994 update was done under the leadership of respected physician and epidemiologist Keiji Fukuda who at that time was with the CDC. The Holmes and the Fukuda definitions were developed for research not clinical purposes: the Fukuda definition (also called Fukuda criteria) is still used for selecting participants in some research. The Fukuda definition requires prolonged fatigue plus four of eight other symptoms.
One of the main criticisms of this definition is that it does not require post-exertion malaise – now widely recognized as the disease’s hallmark symptom — as a mandatory requirement. In other words, the Fukuda definition includes a very heterogeneous group of people, including those with chronic fatigue that can be explained by other conditions, including mental health conditions.
In 2003 what has become to be known as the Canadian consensus criteria (CCC) was developed and for the first time the combined term myalgic encephalomyelitis/chronic fatigue syndrome was used. The development of the criteria was spearheaded by the National ME/FM Action Network, with terms of reference created by Health Canada. These criteria require an extensive list of symptoms, including post-exertional malaise (PEM), with the symptoms from across a number of body systems.
The criteria were developed for clinical use but have often been used in research. Although the CCC has proven to be very good in identifying ME/CFS cases it has been criticized as being complicated to apply in practice. The CCC is often used by expert/advanced practice healthcare providers to confirm a screening diagnosis made using the IOM/NAM criteria.
In an attempt to move beyond the “chronic fatigue syndrome” label and to incorporate emerging research, in 2011 an international group of experts, some of whom had participated in developing the CCC, put forward a new set of criteria for myalgic encephalomyelitis intended for both clinical and research use. They used the CCC as a starting point but they:
removed the need to wait six months before being diagnosed:
required post-exertional neuroimmune exhaustion, which they called PENE (noted by the IOM report writers as the ICC-ME term for PEM); and
also required symptoms from three symptom categories:
These criteria were hailed by some as a step forward in distinguishing ME from chronic fatigue but they never gained a substantial clinical or research following; although there are some, patients in particular, who are strong advocates and do not feel any other definition both captures their disease and rules out those with chronic fatigue who do not also have the entire symptom complex. These criteria will occasionally be seen in use in research publications and have been recommended by the US Clinician Coalition as an alternate to the CCC for confirming an ME diagnosis (after screening using the IOM/NAM criteria).
Enter the 2015 Institute of Medicine criteria. The criteria were quite similar to the CCC but refined to focus on central symptoms and aimed at making it easier for clinicians who do not focus on ME/CFS patients to make a timely diagnosis. As stated, the CCC is often used by expert physicians to confirm the diagnosis that has been arrived at using the 2015 IOM criteria. The 2011 ICC-ME can also be used to confirm the diagnosis.
NICE (UK National Institute for Health and Care Excellence):
Myalgic encephalomyelitis (or encephalopathy)/chronic fatigue syndrome: diagnosis and management: NICE guideline. Reference number: NG206. Published: 29 October 2021.
This document “covers diagnosing and managing myalgic encephalomyelitis (or encephalopathy) /chronic fatigue syndrome (ME/CFS) in children, young people and adults.” As far as criteria, it is similar to those in the IOM report but it shortens the time before which a diagnosis can be made to three months (from six months) for all ages. The purpose of this change is so patients can get the care they need earlier in their illness.
To download the document from the CareNow website click on the button below:
Currently there is no cure for ME. However, research is actively underway to discover treatments. Because the causes of ME are still under investigation, most of the currently available treatments are aimed at relieving specific individual symptoms. These treatments may require a medical doctor or other allied healthcare practitioners (such as a naturopathic doctor, physiotherapist, etc.).
They can be immensely helpful, as can self-help and self-management approaches. Having a support system in place is also important and this applies whether you are a person with ME or a caregiver for such person.
Many people with ME look beyond the mainstream medical (allopathic) system for assistance. They may look, for example, to complementary or integrative medicine. The US National Institutes of Health has a center specifically designed for Complementary and Integrative Health. Their website: “Complementary, Alternative, or Integrative Health: What’s In a Name? explains terms and some of the modalities. We do not go into this topic further except to say that many with ME do find some of the treatments or suggestions (including dietary changes, supplements, acupuncture and more) helpful. As with any treatment modality, be aware of potential benefits as well as potential risks, and ask questions.
Also included in this section are patient specific precautions related to potential adverse effects related to treatments that were used in the past (and may still be prescribed by some, who may not be familiar with the updated literature in the field of ME).
Depending on your specific situation, there is help for ME and we discuss and provide links to some of it in what follows. The information provided in this section is for informational purposes only, it is not intended to diagnose or to treat ME.
Medical assistance is available for ME but because it is not widely taught in medical school and because it is a multi-system disease, that crosses several specialty domains, you may need to actively seek out health care providers who are knowledgeable and experienced in this area of medicine. We have already noted that there is currently no cure and that treatments offered are symptom based. Even so, these symptom based treatments/interventions can be of assistance.
The US ME/CFS Clinician Coalition, a group of 21 US-based clinicians who specialize in ME/CFS, is extremely positive as to what can be done:
“While there are no definitive diagnostic tests or FDA [US Food and Drug Administration] approved treatments specific to ME/CFS, there are no shortage of interventions a clinician can make to improve patient quality of life and significantly reduce the overall symptomatic burden of ME/CFS.”
Bear in mind that treatment plans need to be individualized, as not every person has the same symptoms or same needs. Given one of the diagnostic criteria for ME is post-exertional malaise, however, everyone with ME will benefit from understanding and learning the concept of energy management and pacing.
This 2019 article, from one of the major health plans in the United States, provides some insight into what individualized care means in practice.
In the UK in 2021, a new guideline for ME/CFS care diagnosis and management was published. This guideline recognizes that ME is complex and requires an interdisciplinary team of healthcare professionals to provide care. The ME/CFS specialist teams that were envisaged:
“consist of a range of healthcare professionals with training and experience in assessing, diagnosing, treating and managing ME/CFS. They commonly have medically trained clinicians from a variety of [specialty domains] (including rheumatology, rehabilitation medicine, endocrinology, infectious diseases, neurology, immunology, general practice and paediatrics) as well as access to other healthcare professionals specialising in ME/CFS. These may include physiotherapists, exercise physiologists, occupational therapists, dietitians, and clinical or counselling psychologists.”
This type of interdisciplinary care team is not yet available in Canada but it does provide a potentially useful target.
Three provinces (Ontario, British Columbia and Nova Scotia) have clinics providing some services for patients with ME – all have lengthy waiting lists, all are for adults and at the time of writing, all are restricted to patients from within the particular province.
In Ontario, the clinic devoted to ME, FM and ES/MCS, the Environmental Health Clinic, is at Women’s College Hospital in Toronto. Doctors practising there are familiar with these conditions and their multi-system nature and are equipped to diagnose them and provide management plans. Due to limited funding, they cannot provide ongoing care.
Nova Scotia’s clinic is at the Integrated Chronic Care Service (ICCS) in Fall River.
British Columbia’s at the Chronic Complex Diseases Program (CCDP) at BC Women’s Hospital in Vancouver.
In what follows, you will find links to a selection of information from trusted sources, aimed at healthcare practitioners but which patients and caregivers might also find informative and helpful.
The educational webinar entitled: Myalgic Encephalomyelitis – Diagnosis, Management and Current Research (September 22, 2021) features three ME specialists from three different countries, UKs Dr. Nina Muirhead, USA’s Dr. Lucinda Bateman and from Canada (and the UK) Dr. Luis Nacul along with patient voice Hilary Robertson of the ME/FM Society of BC. This webinar, created for the Federation of Medical Women in Canada, was developed in partnership by the ME|FM Society of BC and the Interdisciplinary Canadian Collaborative Research Network (ICanCME). It was recorded live on September 22, 2021.
1 In 2021 the journal Mayo Clinic Proceedings published an article authored by 21 clinicians specializing in ME/CFS (the US ME/CFS Clinician Coalition, who we referenced earlier) about best clinical practices for adults with ME/CFS. As the Abstract states, in part:
“This article summarizes their top recommendations for generalist and specialist health care providers based on recent scientific progress and decades of clinical experience. There are many steps that clinicians can take to improve the health, function, and quality of life of those with ME/CFS, including those in whom ME/CFS develops after COVID-19. Patients with a lingering illness that follows acute COVID-19 who do not fully meet criteria for ME/CFS may also benefit from these approaches.”
Mayo Clinic Proceedings
The citation for the article is provided below. The full text version can be found here: Bateman L., Bested A.C., Bonilla H.F., Chheda B.V., Chu L., Curtin J.M., Dempsey T.T., Dimmock M.E., Dowell T.G., Felsenstein D., et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Essentials of Diagnosis and Management. Mayo Clin. Proc. 2021;96:2861–2878. doi: 10.1016/j.mayocp.2021.07.004.
2. Authored by Canadian physicians Alison Bested and Lynn Marshall the article dates from 2015. Its diagnosis and management suggestions are based on the Canadian Consensus Criteria (CCC) and remain accurate and timely. Supplemental material including the Functional Capacity Scale and Activity log, as well as to the CCC check list are all most useful for both clinicians and patients. Bested, A. C., & Marshall, L. M. (2015).
Review of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: an evidence-based approach to diagnosis and management by clinicians. Reviews on environmental health, 30(4), 223–249. https://doi.org/10.1515/reveh-2015-0026
Not everyone with ME will need to apply for financial assistance as a result of disability, but many will. Some people are significantly disabled by their illness and cannot continue working and they will need to apply for long term disability programs offered through their employment and/or through the Canadian Pension Plan.
Some may need to apply for provincial disability assistance — in Ontario this is through the Ontario Disability Support Program.
The National ME/FM Action Network has a helpful reference in their CPP Disability guide.
Almost all the disability assistance requires some certification from a healthcare professional.
This guide, Community and Financial Resources, was prepared by the BC Chronic Complex Diseases Program (CCDP) for people in the province of British Columbia but it may provide some ideas for people living in other provinces of the type of support that might be available. There are sections in this guide that are applicable across the country.
We have this as a separate heading to ensure that people with ME and their caregivers pay very close attention. Although exercise is important for most, it may not be beneficial for people with ME, or as a minimum will need to be engaged in with great caution.
As previously mentioned, in 2021 the United Kingdom’s National Institute for Health and Care Excellence (NICE) published a new guideline for the diagnosis and management of ME/CFS. This guideline made special negative mention of both CBT [cognitive behavioural therapy] and GET [graded exercise therapy], with a note that the therapies (as defined in the document) should not be used as a treatment of ME.
The Mayo Clinic Proceedings peer reviewed article on Diagnosis and Management of ME/CFS has a special section discussing the outdated standard of care represented by graded exercise therapy (GET) and cognitive behaviour therapy (CBT). These therapies were previously recommended based on the premise that ME was a condition rooted in false illness beliefs and deconditioning rather than the present understanding of it as a biomedical illness.
In their May 1, 2018 letter to healthcare providers, the Workwell Foundation noted: “Our experiences working with ME/CFS patients are that graded exercise aimed at training the aerobic energy system, not only fails to improve function, but is detrimental to the health of patients and should not be recommended.” The UK patient-focussed organization Action for ME states about graded exercise therapy that: “The information we share about graded exercise therapy (GET) is not a recommendation.”
There are several ways to learn self-management, including courses, books, online. Programs listed below are not all free of cost, therefore it is important to review content carefully before proceeding to assess if you feel the program may be of benefit.
Many local health authorities may offer courses in your area or online, so check and see if there are any in your area. Most of the courses available are geared for chronic illness in general and are not specific to ME. In Ontario, there are both in person and online self-management programs.
Taking the basic skills of self-management and applying them to ME, a number of patients from across Canada, under the medical guidance of Dr. Eleanor Stein (see below for more about Dr. Stein) developed a program dealing with ME: ME/CFS – Living with Myalgic Encephalomyelitis (Chronic Fatigue Syndrome) – Patients helping patients. This course was originally offered in person in Calgary. It has been turned into a series of three videos. The videos are: Defining ME, Self-Management and A Life worth living. These videos, and links to slides and resources, can be found here.
Self-management is very empowering and learning the skills involved is very useful for any chronic illness. ME is no exception. Self-management means observing and learning how the disease affects you, and figuring out if there are things that you can do that will improve how you feel or how you manage and cope with the illness.
It is important, when reading or listening to the experiences of others, to remember that everyone is an individual, so something that works for others may not work for you and conversely, you may be helped by something that does not work for others.
Three more links that you may find useful for self-management are:
“A support system is a group of people who provide you with mental, emotional, and practical support when you need it most. They also keep you going strong when you are doing well.”
Support systems are extremely important for people living with ME. They are also important for their caregivers, particularly so, if the person being cared for is severely or very severely affected. In this section we provide some links relevant for people living with ME as well as some links relevant for caregivers. We end the section with some crisis resources.
“A support system is a group of people who provide you with mental, emotional, and practical support when you need it most. They also keep you going strong when you are doing well.”
Support systems are extremely important for people living with ME. They are also important for their caregivers, particularly so, if the person being cared for is severely or very severely affected. In this section we provide some links relevant for people living with ME as well as some links relevant for caregivers. We end the section with some crisis resources.
The Solve ME/CFS Initiative notes:
“It is crucial to have a personal support system of family, friends, or caregivers to help you through this difficult, debilitating disease. It is important that this support system understands what you are going through so they can help in supportive, empathetic ways.
They go on to issue a bit of a caution, which we repeat, as a reminder – “it can be difficult to find reliable information and avoid misinformation.”
Support groups can be very important in providing a sense of community as you deal with the chronic illness that is ME. Here is what the website ME/CFS & Fibromyalgia Self-Help has to say:
“Support groups can be a crucial coping resource when you have a serious illness. Contact with fellow patients counteracts isolation and provides an experience of being acknowledged and supported. Such contact can be a way to feel understood, comforted and inspired.”
They also caution that not all support groups are created equal — and that it is important that you have a sense of belonging and that you have a positive experience.
A very good article from 2017 (but timeless) is about the importance of connection. It comes from the ME Action website.
It is worth noting that while the websites listing specific support groups endeavour to keep the information up-to-date, it is not always possible – the information can change quickly and without notice.
The American Myalgic Encephalomyelitis and Chronic Fatigue Syndrome Society, a US non-profit set up to provide support and practical advice for ME and CFS patients, lists a number of support groups available for people with ME/CFS that are available online or through the phone. These listings can be found here.
From their list, we highlight two —
Other Canadian places where you might find more information about support or support groups are through the websites of:
Additional sources of information and support include:
Just as a support system is important for the person living with ME, it is also something that caregivers may find helpful as well.
The American Myalgic Encephalomyelitis and Chronic Fatigue Syndrome Society has some resources specific to ME on their website. More general background and information can be found in a number of locations on the web, including this example from the Mayo Clinic.
In Ontario, support resources are available through the website of the Ontario Caregiver organization.
Canada — In Crisis? Call Talk Suicide Canada 1-833-456-4566.
In Quebec 1-866-277-3553. Kids Help Phone 1-800-668-6868.
United States — Crisis resources can be found here.
While there is no Canadian study that looks directly at the economic and social impact of ME, we can learn a lot from studies that have been conducted elsewhere: the UK, the US, Australia and Ireland. And we can supplement these findings with information from the Canadian Community Health Survey (CCHS), much of which is analyzed and reported by the National ME/FM Action Network in a number of their Quest newsletters. An excellent example of this work is contained in Quest 112, from Fall 2017, Special Issue: Under-served and in Great Need.
The bottom line of all this research and information is that ME has a very big economic and social impact, on individuals and also on their caregivers, on their families and on society as a whole.
The level of disability with ME is substantial and can vary from mild to very severe, with approximately 25% housebound. A US multi-clinic study found that up to 75% of people with ME are unable to work. Our (CCHS) data, while not looking directly at the bedbound or housebound aspects, show high percentages (close to 50%) of those with ME needing help with tasks. However, it did not explore how much help was needed. CCHS data from 2014 showed that more than 40% of people with ME were not employed, with about 25% permanently unable to work. We know from both the literature and from the CCHS data that the impacts are substantial at an individual level. Given the large numbers with ME, this has a substantial impact on the economy and at a societal level as well.
Early studies in the UK and US on the economic impact of ME/CFS found it was substantial and composed of individual expenses as well as costs to the healthcare system.
An Australian study published in 2020 found that the economic impact of ME in Australia was estimated at $14.5 billion with “70% due to lost income, 24% due to direct personal OPP [out of pocket] costs on health and medical expenditure, and 6% incurred as a cost to government and the health care system.”
“For direct OOP and Government health care expenditure, high average costs were related to medical practitioner attendance, diagnostics, natural medicines, and device expenditure, with an average attendance of 10.6 referred attendances per annum and 12.1 GP visits per annum related specifically to managing ME/CFS.”
An Irish study also from 2020 found “ME/CFS patients face a wide range of costs, while there are also wider societal costs in the form of costs to the health service, lost productivity, and impacts on informal [caregivers].”
We know that the basic situation is the same here as in other countries – ME is a costly disease for the individual (loss of employment and out of pocket health-related expenses, and high levels of disability) and for the healthcare system.
The CCHS once again provides us with some information, and shows high levels of consultations with both family doctors and with specialists.
Canadian prevalence figures are higher than many other countries, with between 1.4% and 1.9% of the population stating they had been diagnosed by a healthcare professional with ME (called CFS in the survey). What is also notable is that ME impacts many people who are of working age, a large proportion of whom are permanently unable to work.
ME research has been underfunded for decades in the US and elsewhere (including in Canada), but in spite of this, there are many promising research leads and a renewed sense of being on the verge of some big breakthroughs. In 2019, the Canadian Institutes of Health Research funded a research network for ME with the hope that biomedical research would result in an improved quality of life for people living with ME. The ICanCME Research Network is a small start in this direction.
Research is ongoing in many areas and in many countries. Dr. Anthony Komaroff has been involved in the field for decades as both a physician and a researcher. In 2021 he was asked what stood out for him. He replied: “The underlying biological abnormalities in ME that seem to me the most well established involve the brain and autonomic nervous system, chronic activation and exhaustion of parts of the immune system, defects in energy metabolism and a general hypometabolic state, and abnormalities of the gut microbiome. I think it is likely that they are all real, and all connected to one another. To me, the most important research agenda is to understand how these abnormalities are connected to each other.”
Dr. Komaroff’s response does not cover all the research that is taking place into ME, but it gives an indication of how wide-ranging it is. There is every reason to be hopeful.
When COVID-19 first emerged as a health issue, many in the ME community predicted that it would result in a post-infectious condition similar to ME in many cases. This was because many people with ME developed their condition after an infectious illness.
This prediction has proven to be the case with up to 50% of long COVID meeting cases presenting with a similar symptom profile to ME (post exertional malaise, extreme fatigue and activity reduction, sleep disruption, cognitive impairment and/or dysautonomia) and are meeting ME case criteria.
A January 2023 review of long COVID entitled Long COVID: major findings, mechanisms and recommendations draws many of the same parallels and suggests, as have other articles, that long COVID research and care can draw upon lessons already learned in the ME community.
Patient associations, including the US Solve ME/CFS, are working actively with the long COVID community. In the UK the ME Association put out a booklet on long COVID in May 2022. “The [UK] ME Association (MEA) takes the view that Long Covid and ME/CFS are both examples of a serious and debilitating condition that can follow any type of viral infection.”
The ME community is hopeful that research into long COVID will be helpful in arriving at answers for ME and other similar illnesses, and many articles including this one from November, 2022 are appearing, suggesting that the injection of research funds for long COVID may have positive impacts on unravelling the mysteries of ME and will contribute to improved care.
Please also see the information in the Long COVID section on the overlaps with ME. This is an emerging area with more that will be learned, of benefit to both diseases.
Centers for Disease Control and Prevention (CDC) — Myalgic Encephalomyelitis/Chronic Fatigue Syndrome web pages. The CDC has a large informational site for the public and for healthcare providers including toolkits that can be downloaded and links to educational resources. We have referred to some of this material in our ME webpage.
Canadian Institutes of Health Research – Institute of Musculoskeletal Health and Arthritis (IMHA) Online Resource Library
Scroll down to the section on Myalgic Encephalomyelitis (ME). It lists international, national, provincial and local organizations dedicated to supporting people with ME. As well it contains links to useful websites, articles, videos and other resources.
None of the references in this link are from post 2017 and it does not include mention of the 2015 IOM/NAM report on ME/CFS.
Interdisciplinary Canadian Collaborative Myalgic Encephalomyelitis Research Network (ICanCME) – (website under development)
A CIHR-funded national network of researchers, clinicians and patient partners dedicated to advance the understanding of myalgic encephalomyelitis.
See A Conversation about Myalgic Encephalomyelitis with Dr. Nina Muirhead, a CIHR-IMHA webinar, March 16, 2021 – ICanCME Research Network Youtube channel.
Open Medicine Foundation funds research within five ME/CFS Collaborative Research Centres (CRCs) at:
Interdisciplinary Canadian Collaborative Myalgic Encephalomyelitis Research Network (ICanCME) was established in September 2019 through a Catalyst Network grant funded by the Institute of Musculoskeletal Health and Arthritis (IMHA) of the Canadian Institutes of Health Research (CIHR).
Nova Southeastern University – Florida, Institute for NeuroImmune Medicine (INIM) Research and treatment center for neuro-immune disorders including chronic fatigue syndrome and Gulf War Illness.
Simmaron Research ‘Scientifically redefining ME/CFS’ – Non-profit ME/CFS research organization building on the 40-year biobank of Dr. Daniel Peterson
Stanford ME/CFS Initiative – Clinical research to improve diagnosis and treatment of ME/CFS
University of Alabama At Birmingham — Neuroinflammation, Pain and Fatigue Laboratory – Jarred Younger
Each of these clinics has a waiting list, in some cases it is well over a year in length. None of these clinics provide ongoing care al all are geared to the adult population.
British Columbia – The Complex Chronic Diseases Program (CCDP) was established in 2013 at the BC Women’s Hospital in Vancouver as a referral centre for the province of BC.
Referrals to this program are for people over 19 and resident in BC and are made by primary healthcare professionals. The program has “a mandate for care, education/knowledge transfer, and quality improvement/research for complex chronic diseases, including ME/CFS, FM and Alternately Diagnosed Chronic Lyme Syndrome.”
Nova Scotia – Integrated Chronic Care Service – Nova Scotia Health Authority (ICCS, formerly known as the Nova Scotia Environmental Health Centre) has roots that go back to 1996 and is located at Fall River, Nova Scotia.
As a result of service demand, this service is only available by referral from primary care providers from within Nova Scotia. “The ICCS is an interdisciplinary team that provides short term support for individuals diagnosed with or presenting with symptoms of Chronic Fatigue Syndrome/Myalgic Encephalomyelitis, Fibromyalgia (FM) and/or Multiple Chemical Sensitivity/Environmental Illnesses. (The) team provides comprehensive assessment recommendations and short-term interventions focused on self-management.”
Ontario – Environmental Health Clinic – (EHC) was established by the provincial government,ent in 1996 and is located at Women’s College Hospital in Toronto.
Referrals to the clinic are from primary healthcare providers. The clinic was established as “a provincial resource in promoting environmental health and to promote health care for people with chronic environmentally-linked conditions such as Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS), Fibromyalgia Syndrome (FM) and Environmental Sensitivities (ES/MCS) and Electromagnetic Hypersensitivity.”
Open Medicine Foundation Canada has a large resource Information section, called: “for your doctor“.
Bateman Horne Center — Is a non-profit Center of Excellence for research, clinical care and education for patients with multi-system complex diseases (msCCD). Many resources, including video, are available for patients and clinicians. We have referred to many of these on our ME webpage. It is home to a Medical Education Resource Center. It Has a full video library on their Youtube channel
Educational videos from Dr. Eleanor Stein (Calgary, Alberta). Three short educational videos explaining i) What ME is, ii) How to diagnose it, and finally iii) helpful management strategies. The videos are based on material prepared for educating medical students at the University of Calgary.
U.S. ME/CFS Clinician Coalition — Website contains a wealth of information on diagnosis and treatment, including a translation of their 2019 handout on the Basics of Diagnosis and Treatment in French, Italian, Spanish, German, Portuguese and Danish. We will be or have referred to some of this information in our ME webpage.
American Myalgic Encephalomyelitis and Chronic Fatigue Syndrome Society
American Myalgic Encephalomyelitis and Chronic Fatigue Syndrome Society: Physician and Clinic Database – “a compilation of clinicians in the United States who have treated patients with ME and CFS.” As a note, although data can quickly get out of date, this may provide a helpful starting point for people in the United States or for those able to travel.
Drs with ME — Doctors with ME is the global professional association for medical practitioners and scientists with backgrounds developed in hospitals, surgeries, universities, financial services and think-tanks and with lived experience with ME or who stand with Doctors with ME. The website provides information and position papers related to ME and to long COVID.
IACFSME – International organization dedicated to the care and research of people affected by ME/CFS and related disorders.
Open Medicine Foundation Canada – A Canadian charity “driving research of ME/CFS, Post Treatment Lyme Disease Syndrome (PTLDS), Fibromyalgia and Post COVID.” The charity focuses on chronic complex disease research, collaborating with leading scientists and clinicians from around the world.
A US charity, Open Medicine Foundation, exists for the same purposes.
Physios for M.E. is a group of physiotherapists in the United Kingdom with a special interest in Myalgic Encephalomyelitis (ME) who aim to educate and advocate. Website has educational material.
Solve M.E. (Solve ME/CFS initiative) — “The Solve ME/CFS Initiative (Solve M.E.) is a non-profit organization that serves as a catalyst for critical research into diagnostics, treatments, and cures for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), Long Covid and other post-infection diseases.”
25% M.E. Group is a U.K. based charity raising awareness about severe ME. Its webpage has links to a number of resources for people with severe myalgic encephalomyelitis and for their carers.
Millions Missing Canada – Advocates for treatment access, appropriate medical care and equitable research funding for ME in Canada and
the ME/FM Society of British Columbia.
National ME/FM Action Network – Lots of useful information including the CPP disability guide, a sourcebook for teachers and parents, information on statistics and a quarterly newsletter Quest
ME/FM Society of BC – works to support ME and FM patients in BC to improve their health and quality of life by providing information about these illnesses. They also inform and educate health professionals and raise awareness with the general public and government. Their website contains information on a variety of subjects including the recently complete Convene project looking at the unmet needs of British Columbians living with Myalgic Encephalomyelitis
Association Québécois de l’Encéphalomyélite Myalgique — Website and resources in French
#ME ACTION — “An international organization working to develop and support a global network of individual advocates, local groups, city and state chapters, and country affiliates” whose mission is to fight for recognition, education and research. The website contains many resources for people with the condition, their caregivers and healthcare providers.
Science for ME – an independent, patient-led, international forum for anyone interested in ME/CFS – patients, carers, scientists, educators, clinicians, advocates. The forum contains postings and thoughtful discussions about many scientific topics or other topics of direct relevance including support and advocacy.
World ME Alliance — An alliance of national ME organizations that aims to bring ME out of the shadows.
American Myalgic Encephalomyelitis and Chronic Fatigue Syndrome Society – Its webpage contains a wealth of information about ME/CFS, treatments and support
Health Rising: Health Rising’s goal is the eradication of ME/CFS and FM by sharing the latest research, treatment and advocacy news. Founder Cort Johnson and guest bloggers share and analyze the latest in promising research.
Phoenix Rising: Phoenix Rising is an non-profit provides support and community to people with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), as well as related conditions. They maintain a community forum for exchange of information.
Invest in ME Research: commissions and funds biomedical investigation into ME/CFS
ME Research UK: funds high-quality biomedical research into ME.
2021 — Bateman, L., Bested, A. C., Bonilla, H. F., Chheda, B. V., Chu, L., Curtin, J. M., Dempsey, T. T., Dimmock, M. E., Dowell, T. G., Felsenstein, D., Kaufman, D. L., Klimas, N. G., Komaroff, A. L., Lapp, C. W., Levine, S. M., Montoya, J. G., Natelson, B. H., Peterson, D. L., Podell, R. N., Rey, I. R., … Yellman, B. P. (2021). Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Essentials of Diagnosis and Management. Mayo Clinic Proceedings 96(11), 2861–2878.
2015 — Bested, A. C., & Marshall, L. M. (2015). Review of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: an evidence-based approach to diagnosis and management by clinicians. Reviews on environmental health, 30(4), 223–249.
Jason LA, Katz BZ, Sunnquist M, Torres C, Cotler J, Bhatia S. The Prevalence of Pediatric Myalgic Encephalomyelitis/Chronic Fatigue Syndrome in a Community‑Based Sample. Child Youth Care Forum. 2020 Aug;49(4):563-579. doi: 10.1007/s10566-019-09543-3. Epub 2020 Jan 23. PMID: 34113066; PMCID: PMC8186295.
Rowe, P. C., Underhill, R. A., Friedman, K. J., Gurwitt, A., Medow, M. S., Schwartz, M. S., Speight, N., Stewart, J. M., Vallings, R., & Rowe, K. S. (2017). Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Diagnosis and Management in Young People: A Primer. Frontiers in pediatrics, 5, 121.
Canadian Consensus Criteria and treatment protocols (2003) Carruthers BM, Jain AK, De Meirleir KL, Peterson DL, Klimas NG, Lerner AM, Bested AC, Flor-Henry P, Joshi P, Powles ACP, Sherkey JA, van de Sande MI. Myalgic Encephalomyelitis/chronic fatigue syndrome: Clinical working case definition, diagnostic and treatments protocols. J Chronic Fatigue Syndr. 2003;11:7–115
US Institute of Medicine, now the Academy of Medicine, (2015) Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. This is a book that can be read on-line.
UK National Institute for Health and Care Excellence (NICE) guidance (2021) Press release on the launch of the new guidance, with quotes https://www.nice.org.uk/news/article/nice-me-cfs-guideline-outlines-steps-for-better-diagnosis-and-management”
Myalgic encephalomyelitis (or encephalopathy)/chronic fatigue syndrome: diagnosis and management. NICE guideline [NG206] Published 29 October, 2021. https://www.nice.org.uk/guidance/ng206 The guideline includes advice on diagnosis and management for ME/CFS, including for severe and very severe cases.
Montoya JG, Dowell TG, Mooney AE, Dimmock ME, Chu L. Caring for the Patient with Severe or Very Severe Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Healthcare (Basel). 2021 Oct 6;9(10):1331. doi: 10.3390/healthcare9101331. PMID: 34683011; PMCID: PMC8544443. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8544443/
Carruthers, B. M., van de Sande, M. I., De Meirleir, K. L., Klimas, N. G., Broderick, G., Mitchell, T., Staines, D., Powles, A. C., Speight, N., Vallings, R., Bateman, L., Baumgarten-Austrheim, B., Bell, D. S., Carlo-Stella, N., Chia, J., Darragh, A., Jo, D., Lewis, D., Light, A. R., Marshall-Gradisnik, S., … Stevens, S. (2011). Myalgic encephalomyelitis: International Consensus Criteria. Journal of internal medicine, 270(4), 327–338.
Chang C-J, Hung L-Y, Kogelnik AM, Kaufman D, Aiyar RS, Chu AM, Wilhelmy J, Li P, Tannenbaum L, Xiao W, Davis RW. A Comprehensive Examination of Severely Ill ME/CFS Patients. Healthcare. 2021; 9(10):1290.
Montoya JG, Dowell TG, Mooney AE, Dimmock ME, Chu L. Caring for the Patient with Severe or Very Severe Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Healthcare (Basel). 2021 Oct 6;9(10):1331. doi: 10.3390/healthcare9101331. PMID: 34683011; PMCID: PMC854444.
Bested, A. C., & Marshall, L. M. (2015). Review of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: an evidence-based approach to diagnosis and management by clinicians. Reviews on environmental health, 30(4), 223–249.
Hng, K. N., Geraghty, K., & Pheby, D. (2021). An Audit of UK Hospital Doctors’ Knowledge and Experience of Myalgic Encephalomyelitis. Medicina (Kaunas, Lithuania), 57(9), 885 https://doi.org/10.3390/medicina57090885
Jason, L.A., Taylor, R.R., Plioplys, S., Stepanek, Z., & Shlaes, J. (2002). Evaluating attributions for an illness based upon the name: Chronic fatigue syndrome, myalgic encephalopathy and Florence Nightingale disease. American Journal of Community Psychology, 30, 133—148
Komaroff, A. (2019). Advances in Understanding the Pathophysiology of Chronic Fatigue Syndrome. JAMA. Published online July 5, 2019. Doi:10.1001/jama.2019.8312 https://jamanetwork.com/journals/jama/fullarticle/2737854 subscription only