
working to improve care for people living with:
Most family doctors in Ontario have probably heard of Fibromyalgia but may not have experience diagnosing or treating it. It is not uncommon for people living with Fibromyalgia to have waited years for a diagnosis. The (Canadian) Centre for Effective Practice or CEP has created a tool to help family physicians recognize, assess, diagnose and treat Fibromyalgia. To access the tool click on the blue button: “CEP Tools for Fibromyalgia”. Bring this tool to the attention of your doctor.
The CEP is a Canadian group focused on helping Canadian primary care clinicians (like your family doctor) “navigate the increasingly complex clinical environment”. In other words they offer Canadian doctors guides to cope with the ever-changing world of medical practice. A great example of this is the aforementioned “tool” designed to help your doctor diagnose and treat Fibromyalgia.
The CEP has also prepared a list of resources for both patients and clinicians. Click on the respective blue buttons for copies of these resources.

Fibromyalgia is recognized by the medical discipline of Rheumatology as a real condition. Rheumatologists have written extensively on the subject and have created diagnostic criteria that can be used by general practitioners of medicine: you can get a diagnosis from your family doctor. It is characterized by nociplastic pain which appears to originate in the brain (central nervous system) and is not a consequence of acute threats to tissue (nociceptive pain) nor caused by damage to nerves (neuropathic pain). There are a number of other common symptoms including fatigue, sleep disturbances, cognitive dysfunction, and depression and anxiety. There is help for people suffering from Fibromyalgia. While there is no cure there are both pharmacological and non-pharmacological “treatments” that can help manage symptoms. The Ontario based Centre for Effective Practice (a Canadian organization that “helps primary care clinicians navigate the increasingly complex clinical environment”) has created a set of tools that your doctor can use to both diagnose and treat Fibromyalgia.
“Fibromyalgia is characterized by chronic widespread pain, fatigue, sleep disturbances and functional symptoms.” It is estimated that 3.3% of Canadians have the condition afflicting 3 times as many women as men (1).
It is considered to be a rheumatological disorder.
Fibromyalgia is the third most frequent Musculoskeletal condition, and its prevalence increases with age.
Rheumatologists have written extensively on the subject and have created diagnostic criteria that can be used by family doctors.
“Although diagnosis has improved with the evolution of more accurate diagnostic criteria, a considerable proportion of physicians still fail to recognize the syndrome.” (1)
Statistics Canada reports that the prevalence of the condition in Canada is less than 2% but this probably reflects that fact that many with the condition go un-diagnosed.
The British Royal College of Physicians (RCP) describes Fibromyalgia syndrome (FMS) as a condition characterised by persistent and widespread pain that is associated with intrusive fatigue, sleep disturbance, impaired cognitive and physical function and psychological distress. (2) The RCP goes on to say that Fibromyalgia is not.
It is not a condition caused by:
AND it is not “all in the head’” (2)
Closer to home the Ontario based Centre for Effective Practice or CEP describes Fibromyalgia as “a disease characterized by widespread musculoskeletal pain (pain in bones, muscles, tendons, ligaments, cartilage, and joints) which is nociplastic in nature and can be very disabling, Other key symptoms are disturbed sleep, fatigue, and impaired cognitive and physical function. Symptoms vary from person to person and may fluctuate from day to day.” (3)
The CEP is a Canadian organization that “helps primary care clinicians navigate the increasingly complex clinical environment”. It has produced a tool to help Canadian doctors diagnose and treat Fibromyalgia. If you live in Ontario your doctor will probably have heard of the CEP and will probably be willing to use the tool that it has created. In this case the term “tool” refers to a set of guidelines designed to educate primary care clinicians (like your GP) regarding the diagnosis and treatment of Fibromyalgia. Here is a link to the tool which you can share with your primary care providers: https://tools.cep.health/tool/fibromyalgia/
It should be noted that the CEP tool calls up a diagnostic “worksheet” published by the British Royal College of Physicians.
It also calls up the “2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria” which represent the current consensus with respect to diagnostics (4). This document is referred to extensively in the section 2 entitled Diagnostic Criteria.
We have a copy of that paper.
The International Association for the Study of Pain has offered the following definition of pain:
“Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.”
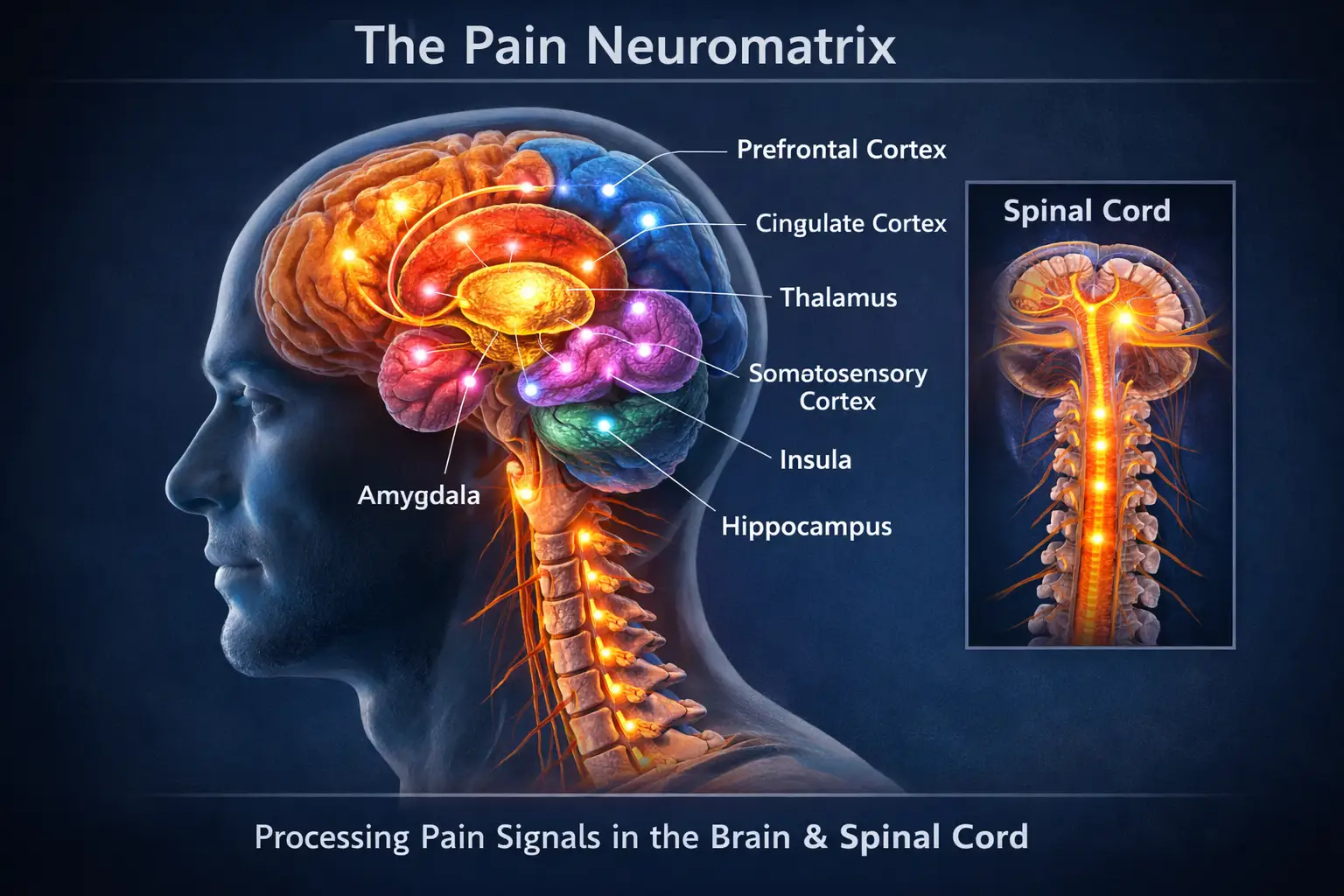
Processing of pain is quite complex involving over a dozen specific regions of the brain and spinal column. This network of brain structures has been referred to as the “neuromatrix” which “processes sensory input and output neural impulses which influence sensing and perception of pain. (5)
Pain can be classified as nociceptive (pain that alerts us to actual or imminent tissue damage such as heat that could -or has already- caused a burn), neuropathic (caused by nerve damage), and nociplastic (a consequence of aberrations in the way pain is processed by the brain). ”Nociplastic” is the primary form of pain in Fibromyalgia. (2)
Nociceptors are found in skin, joints, viscera, and muscles. They alert us to dangers such as extreme temperatures, or pressure, that could cause or have caused tissue damage (6). We experience this as pain. Grab the handle of a pot that is too hot and you immediately experience nociceptive pain. Fibromyalgia is characterized by nociplastic pain not nociceptive pain.
Fibromyalgia is characterized by nociplastic pain.
It has only been in the past decade that the notion of nociplastic pain has gained acceptance. It is pain that is not a consequence of acute threats to tissue (nociceptive pain) nor caused by damage to nerves (neuropathic pain). The specific cause of nociplastic pain is not yet understood but it is thought to be a consequence of changes in pain-related sensory pathways in the Peripheral Nervous System and Central Nervous System (the brain and spinal column), causing increased sensitivity or -in plain English- due to some changes to the complex way pain is processed by the brain, or to the pathways along which pain signals are sent.
For example nociplastic pain may be a consequence of pain amplification by the brain or the failure of the brain to inhibit pain adequately. Thus pain that should be either mild or non-existent is experienced as severe and widespread.
It is also possible that people who experience nociplastic have become far more sensitive to pain stimuli (7).
Nociplastic pain is, thus, thought to be a condition driven by the nervous system rather than pain receptors (nociceptors) (8)
The British Royal College of Physicians simply describes it as “abnormal pain processing within the nervous system”. (2)
The term nociplastic pain “provides validity for pain complaints previously identified by stigmatising terms such as dysfunctional pain or medically unexplained somatic syndromes” (7). In essence the research community and the medical profession recognize that the pain experienced by people with Fibromyalgia is real and not simply a psychological phenomenon.
Key symptoms of nociplastic pain include:
The theory is that these symptoms: widespread pain, fatigue, sleep disturbances, cognitive dysfunction, and mood issues are all problems of the central nervous system.(7)
“Nociplastic pain was recently endorsed as the third mechanistic descriptor of pain and is characterized by widespread body pain, often co-occurring with fatigue and altered sleep, cognition and mood, as well as multisensory hypersensitivity.”(9) This means that the medical community now accepts that nociplastic pain is real and is not caused by nerve damage or pain sensors.
These symptoms of nociplastic pain are also the common symptoms of Fibromyalgia. Fibromyalgia involves nociplastic pain.
(other medical conditions that people with Fibromyalgia often have)
People with Fibromyalgia often have chronic ME/CFS, irritable bowel syndrome, anxiety disorders, and sleep disorders as well as other chronic pain conditions such rheumatoid arthritis and osteoarthritis, These comorbidities may arise from central sensitization mechanisms, but not all associations can be explained by this (10). Just keep in mind that the term “central sensitization” is often used to describe what has happened to people with Fibromyalgia.
[1] Sarzi-Puttini P, Giorgi V, Marotto D, Atzeni F. Fibromyalgia: an update on clinical characteristics, aetiopathogenesis and treatment. Nat Rev Rheumatol. 2020 Nov;16(11):645-660. doi: 10.1038/s41584-020-00506-w. Epub 2020 Oct 6. PMID: 33024295.
[2] Royal College of Physicians. The diagnosis of fibromyalgia syndrome. UK clinical guidelines. London: RCP, 2022.
[3] Centre for Effective Practice (CEP): Fibromyalgia
[4] Frederick Wolfe, Daniel J. Clauw, Mary-Ann Fitzcharles, Don L. Goldenberg, Winfried Häuser, Robert L. Katz, Philip J. Mease, Anthony S. Russell, Irwin Jon Russell, Brian Walitt, 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria, Seminars in Arthritis and Rheumatism, Volume 46, Issue 3, 2016, Pages 319-329, ISSN 0049-0172, https://doi.org/10.1016/j.semarthrit.2016.08.012.
[5] Melzack R. From the gate to the neuromatrix. Pain. 1999 Aug;Suppl 6:S121-S126. doi: 10.1016/S0304-3959(99)00145-1. PMID: 10491980.
[6] Sarah Kendroud; Lauren A. Fitzgerald; Ian V. Murray; Andrew Hanna. Physiology, Nociceptive Pathways StatPearls Publishing January 2025.
[7] Fitzcharles MA, Cohen SP, Clauw DJ, Littlejohn G, Usui C, Häuser W. Nociplastic pain: towards an understanding of prevalent pain conditions. Lancet. 2021 May 29;397(10289):2098-2110. doi: 10.1016/S0140-6736(21)00392-5.
[8] Clauw D, Sarzi-Puttini P, Pellegrino G, Shoenfeld Y. Is fibromyalgia an autoimmune disorder? Autoimmun Rev. 2024 Jan;23(1):103424. doi: 10.1016/j.autrev.2023.103424. Epub 2023 Aug 25. PMID: 37634681.
[9] Kaplan CM, Kelleher E, Irani A, Schrepf A, Clauw DJ, Harte SE. Deciphering nociplastic pain: clinical features, risk factors and potential mechanisms. Nat Rev Neurol. 2024 Jun;20(6):347-363. doi: 10.1038/s41582-024-00966-8. Epub 2024 May 16. PMID: 38755449.
[10] Arnold LM, Bennett RM, Crofford LJ, Dean LE, Clauw DJ, Goldenberg DL, Fitzcharles MA, Paiva ES, Staud R, Sarzi-Puttini P, Buskila D, Macfarlane GJ. AAPT Diagnostic Criteria for Fibromyalgia. J Pain. 2019 Jun;20(6):611-628. doi: 10.1016/j.jpain.2018.10.008. Epub 2018 Nov 16. PMID: 30453109.
The medical community accepts that Fibromyalgia is real and that the field of medicine that defines the condition is Rheumatology.
Within the medical field of Rheumatology there is agreement regarding what the diagnostic criteria for Fibromyalgia are. They were arrived at by a group of Rheumatologists over a period of years and published in “Seminars in Arthritis and Rheumatism” in 2016. The CEP refers to it as the 2016 revisions to ACR 1990/2010 diagnostic criteria. The following is the full citation for that article. Most of the information in this section (Diagnostic Criteria) is derived from that article.
Frederick Wolfe, Daniel J. Clauw, Mary-Ann Fitzcharles, Don L. Goldenberg, Winfried Häuser, Robert L. Katz, Philip J. Mease, Anthony S. Russell, Irwin Jon Russell, Brian Walitt, 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria, Seminars in Arthritis and Rheumatism, Volume 46, Issue 3, 2016, Pages 319-329, ISSN 0049-0172, https://doi.org/10.1016/j.semarthrit.2016.08.012. (https://www.sciencedirect.com/science/article/pii/S0049017216302086)
Please note that this article is also referenced in the section entitled “What is Fibromyalgia?”
Fibromyalgia patients and non-professional caregivers can make requests for free copies of “this paper” by contacting Elsevier. Here are the instructions. Use the above citation.
Fibromyalgia may now be diagnosed in adults when all of the following criteria are met:
These same diagnostic criteria are used by the CEP.
To arrive at a diagnosis one needs to know:
For the purposes of meeting the first criteria of generalized pain the patient’s body is divided into five regions.
*The Axial region is the central axis, including head, neck, chest and trunk or, in other words, the core of the body that is distinct from the limbs and appendages which include shoulders, pelvis and limbs, including your arms, hands, legs and feet Cleveland Clinic “Axial Skeleton”
A patient must experience pain in four of these five regions with the caveat that pain in the jaw, chest, or abdomen are not counted as being part of any of the regions for the purpose of determining the incidence of generalized pain.
Clinicians look for chronic pain (pain lasting for 3 months or more) in the following 19 locations within the five regions of the body described above.



The number of these locations where a patient has experienced chronic pain are tallied to generate the Widespread Pain Index (WPI).
Fatigue disproportionate to activity performed which is reminiscent of ME/CFS.
Scoring
The minimum score is 0. The maximum score is 3.

Sleep that is unrefreshing, difficulty falling asleep, more frequent nighttime awakenings.
Scoring
The minimum score is 0. The maximum score is 3.

brain or “fibro” fog, memory problems, loss of verbal fluency (difficulty finding the right words)
Scoring
The minimum score is 0. The maximum score is 3.

When added together the minimum score for this set of symptoms is zero and the maximum score is nine.
No=zero, Yes=one
No=zero, Yes=one
No=zero, Yes=one
When added together the minimum score for this set of symptoms is zero and the maximum score is three.
For example severe fatigue (three) plus minor sleep troubles (one) plus minor cognitive problems (one) plus headaches (one) and depression (one) would result in a symptom severity score (SSS) of seven.
Symptoms must have been experienced during the previous six months.
For a diagnosis of Fibromyalgia the WPI must be equal or greater than 7 if the Symptom Severity Scale score is equal to or greater than 5. If the WPI is between 4 and 6 the Symptom Severity Scale score must be equal to or greater than 9. The authors of the diagnostic criteria recognize that symptoms exist upon a continuum but chose these discrete metrics so that clinicians who are not Rheumatologists can arrive at a diagnosis of Fibromyalgia using a reliable method.
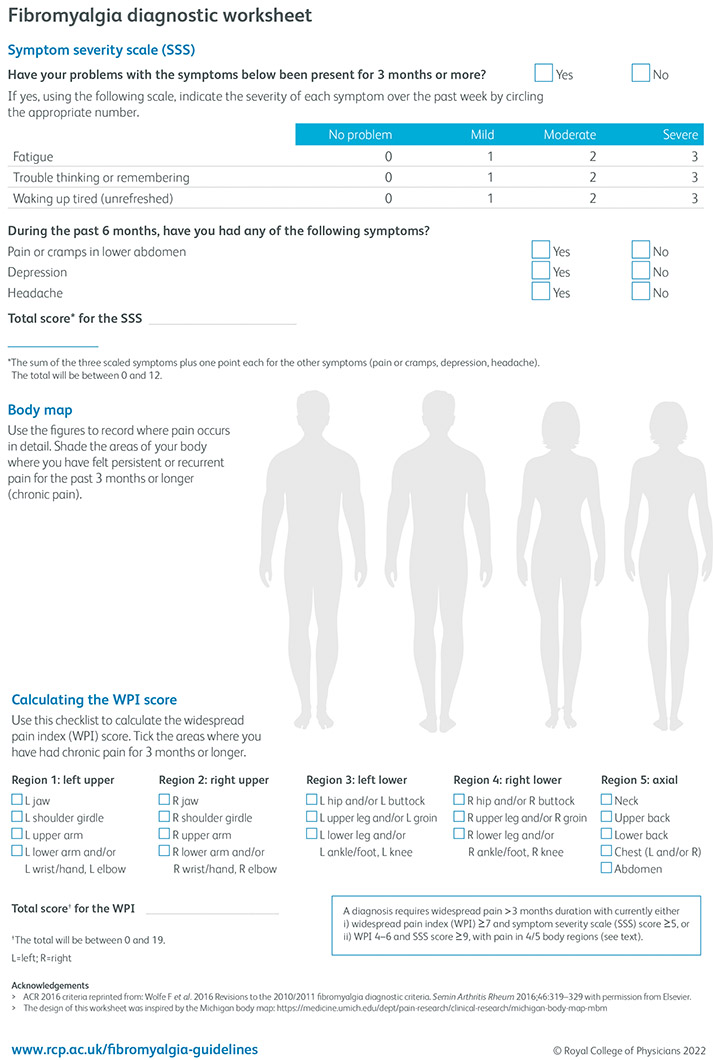
The British Royal College of Physicians has created a diagnostic worksheet for Fibromyalgia.
Click on this link to get a copy of the worksheet.
It looks like this:
There is a consensus among experts that symptoms can change from day to day.
There is no cure for Fibromyalgia but there are strategies that can be employed to manage or alleviate symptoms. The CEP uses the following language: “There is no curative treatment for FM. Management aims to reduce symptom severity and improve the patient’s quality of life.” (1)
“Many factors contribute to the development of fibromyalgia in a unique manner: genetic predisposition, personal experiences, emotional–cognitive factors, mind–body relationship and a biopsychological ability to cope with stress. In this sense, fibromyalgia can be seen as a condition that represents a mind–body hyper-connection, rather than a mind–body disconnection. Consequently, fibromyalgia treatment needs to be holistic and comprehensive. Indeed, the therapeutic approach to managing patients with fibromyalgia is characterized by integrated and multidisciplinary interventions” (2) In other words FM is probably a consequence of many factors and, therefor, treatment needs to be tailored to the individual.
“Treatment should be multimodal and built on four pillars:
The approach should be individualized, symptom-based and stepwise, establishing shared goals with the patient.” [2]
“An important step in managing patients with fibromyalgia is ensuring that the patients understand their illness before they are prescribed any medications. It is crucial to reassure patients that fibromyalgia is a real pathological condition and to legitimize their suffering, making it clear that, although disabling, the condition is not progressive and is not due to peripheral tissue damage.” [2]
This is consistent with the CEP tool for diagnosing and managing Fibromyalgia.
Providing patients with relevant information is considered a key element in treatment/management of Fibromyalgia since patients play a key role in the management of their condition. In particular an understanding of pain and pain management is very important. The CEP references the following three information sources:
1) The British Royal College of Physicians provides extensive information for both physicians and patients with respect to Fibromyalgia; however, like most web sites it gets reorganized now and then leading to broken links. As of this writing the patient information document referred to by the CEP can be found by going to this web site: https://www.rcp.ac.uk/improving-care/resources/the-diagnosis-of-fibromyalgia-syndrome/ click on the plus icon next to “downloads” and select: Fibromyalgia syndrome: the essentials -for patients. Or click on this link:
https://www.rcp.ac.uk/media/mfmpij5t/fibromyalgia-information-sheet-for-patients.pdf
2) Pain U Online: Online learning modules to improve understanding of pain and support self-management approaches to chronic pain.
3) Power over Pain Portal: Virtual chronic pain management portal.
Exercise can help reduce pain. Both aerobic and resistance training is indicated for treating Fibromyalgia with the caveat that if the patient also has ME/CFS (Myalgic Encephalomyelitis/Chronic Fatigue Syndrome) any exertion must be limited by the patients energy budget. If you have ME/CFS exercise can harm rather than help. Any exercise regimen must be tailored to the individual.
The CEP also recommends both occupational therapy (modification of daily activities in a way that increases one’s quality of life) and hydrotherapy (water-based exercise, aquatic physical therapy, thermal therapy).
Pain is distressing. Chronic pain is more distressing. In other words pain causes stress which often has psychological consequences.
Cognitive Behavioural Therapy or CBT is a recommended treatment [3]. It is used for pain management and to help with sleep. CBT is a psychotherapeutic tool. This does not imply that Fibromyalgia is a psychological condition. However, pain does have an emotional component. Recall that the definition of pain is (an) “unpleasant sensory and emotional experience”.
The amygdala is the region of the brain that processes emotions and said region of the brain contributes to the processing and perception of pain [4]. It can both amplify and dampen the experience of pain. It is also true that we describe some emotions in terms of pain -the amygdala is where pain and emotion interact.
One consequence of pain is that it teaches us about danger which often manifests as fear. Don’t do things that might hurt you.
Since nociplastic pain is not well understood a patient who is experiencing it might fear that it is never going away or that it might get worse. This kind of speculation (fear) can cause the experience of pain to be more intense. CBT is a technique whereby we can use our thinking brain to “manage” our fears. In psychotherapeutic terms CBT can help one avoid panic or catastrophization -a tendency to exaggerate the negative and assume the worst possible outcome.
This same notion can be applied to sleep problems where someone who is having difficulty falling asleep starts to think that they will never be able to fall asleep.

Non-conventional therapies to be considered may be:
Category of Evidence
Grade A refers to the strength of a recommendation based on the highest level of evidence. It indicates that the recommendation is supported by robust evidence, typically derived from meta-analyses of randomized controlled trials or at least one randomized controlled trial (Category 1 evidence). This grade signifies strong confidence in the recommendation’s validity and effectiveness. Grades B, C, & D confer ever decreasing levels of credibility
The following list was compiled by the Centre for Effective Practice [6]
May be effective in reducing pain symptoms associated with fibromyalgia. Helps with sleep disrupted by pain symptoms and restless leg syndrome.
Helpful for pain symptoms in fibromyalgia.
Suggested to offer multiple benefits to patients with FM by blocking certain receptors.
Compounded medication, needs to be obtained from a compounding pharmacy.
May improve symptoms in patients with Fibromyalgia. Low-Dose Naltrexone modulates inflammation through various mechanisms including interruption of microglial cell activation within the central nervous system.
[1] CEP Fibromyalgia Tool
[2] Sarzi-Puttini P, Giorgi V, Marotto D, Atzeni F. Fibromyalgia: an update on clinical characteristics, aetiopathogenesis and treatment. Nat Rev Rheumatol. 2020 Nov;16(11):645-660. doi: 10.1038/s41584-020-00506-w. Epub 2020 Oct 6. PMID: 33024295.
[3] Cognitive Behavioral Therapy Eases How Fibromyalgia Pain is Experienced by the Brain which is based on the following research:
Lee J, Lazaridou A, Paschali M, Loggia ML, Berry MP, Ellingsen DM, Isenburg K, Anzolin A, Grahl A, Wasan AD, Napadow V, Edwards RR. A Randomized Controlled Neuroimaging Trial of Cognitive Behavioral Therapy for Fibromyalgia Pain. Arthritis Rheumatol. 2024 Jan;76(1):130-140. doi: 10.1002/art.42672. Epub 2023 Nov 21.work published in Sept 20, 2023
[4] Neugebauer V, Li W, Bird GC, Han JS. The amygdala and persistent pain. Neuroscientist. 2004 Jun;10(3):221-34. doi: 10.1177/1073858403261077. PMID: 15155061.
[5] Ariani A, Bazzichi L, Sarzi-Puttini P, Salaffi F, Manara M, Prevete I, Bortoluzzi A, Carrara G, Scirè CA, Ughi N, Parisi S. The Italian Society for Rheumatology clinical practice guidelines for the diagnosis and management of fibromyalgia Best practices based on current scientific evidence. Reumatismo. 2021 Aug 3;73(2):89-105. doi: 10.4081/reumatismo.2021.1362. PMID: 34342210.
[6] Centre for Effective Practice (CEP): Fibromyalgia
Bateman Horne Centre A centre dedicated to the diagnosis and care of patients with ME/CFS, Fibromyalgia & Long COVID (Diagnostic criteria for Fibromyalgia, provides videos, handouts and health management guidance.)
The Diagnosis of Fibromyalgia Syndrome Royal College of Physicians, UK (Educational resource and information sheet for patients.)
What is Fibromyalgia? (Video) Dr. Andrea Furlan, MD PhD, Toronto (Educational video which discusses causes and treatments for Fibromyalgia.)
Environmental Health Clinic, Women’s College Hospital, Toronto An Ontario-wide provincial resource/clinic for patients who meet the criteria for ME/CFS, FM or ES/MCS. (Assesses patients and supports primary care clinicians in Ontario determining whether their patients meet criteria for ME/CFS, FM or ES/MCS and provides recommendations for management to be carried out by the patient’s primary care provider. Requires a referral from a primary care clinician. Lengthy wait list.)
Complex Chronic Diseases Program (CCDP), BC Women’s Hospital and Health Clinic, Vancouver. (Information to support diagnosis, treatment, and additional educational resources.
Royal College of Physicians (UK)
The diagnosis of fibromyalgia syndrome
https://www.rcp.ac.uk/improving-care/resources/the-diagnosis-of-fibromyalgia-syndrome